

Introduction
Vaso-Occlusive Crisis (VOC), the most common manifestation of sickle cell disease (SCD), is the first cause of death when complicated by an acute chest syndrome (ACS). We previously developed a predictive score for the occurrence of ACS in SCD patients admitted at hospital for a VOC episode (Bartolucci et al., 2016). Two hundred and fifty patients with severe VOC requiring hospitalization were included in the PRESEV I study and 19% developed a secondary ACS within days post-admission (median [IQR] : 3 [2.3]). A multivariate analysis of these data established a predictive score of secondary ACS, with a negative predictive value of 98,9% for the low-level risk. Variables for calculation of the score were: reticulocytes and leucocytes counts, hemoglobin and categorical pain score (spine -pelvis). Interestingly enough, Hydroxyurea treatment did not have any impact on the score. Our goal was to validate this score in a multicenter international study, as it could represent a useful tool for physicians, for improving VOC management, but also be of use for therapeutic trials. Herein, we present results for adults.
Methods
This international, multicenter, prospective, observational study was performed in thirteen centres, over two continents (Africa and Europe) and five countries (Mali, Togo, England, Belgium and France). Homozygous SCD patients, both adults and children (>2 years), were included, with severe VOC requiring admission at the emergency unit. Severe VOC was defined as pain or tenderness affecting at least one part of the body (e.g. limbs, ribs, sternum, head, spine and/or pelvis) requiring opioids (level 3) and not attributable to other causes.
The primary outcome measure was the occurrence of an ACS, defined as an auscultatory abnormality (crepitation or bronchial breathing), or the association of a new radiologic infiltrate and chest pain or decreased breath sounds. Secondary outcome measures were hospital length of stay, morphine consumption, transfusion, hospitalization in intensive care unit and mortality.
The following parameters were recorded: temperature, blood pressure, oxygen saturation, respiratory frequency, categorical pain score. Pulmonary auscultation was performed at least once a day by a physician, every day, for the length of stay. The auscultatory abnormality, defined as crepitation, bronchial breathing or decreased breath sounds, was confirmed by a second physician. If a patient was discharged before day 5, follow-up with a phone call and/or a visit, 3 to 7 days after discharge were performed, to prevent complications or ACS.
Results
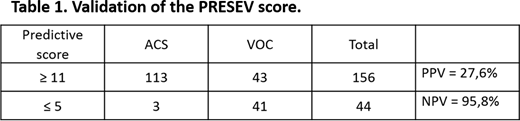
Three hundred and seventy-two adult patients with a severe VOC requiring hospitalization were included. Mean age was 29 (±8) years old, sex ratio (female/male) was 1.2. A hundred and ninety-one patients came from Europe and 181 from Africa. Out of the 372 patients, 68 (18.3%) further developed a secondary ACS. Mean day of ACS episode was 3.3 (±1.37). Among the 304 patients who did not develop an ACS episode (81.7%), 41 had a low risk score of developing a secondary ACS (predictive score ≤ 5). Among the 68 patients who developed a secondary ACS, 43 had a high-risk score (≥ 11). Results are shown in table 1. Three deaths were reported, all on African continent (ACS, anemia and end-stage nephropathy).
Discussion and Conclusion
Our multicenter international study has allowed confirmation of the incidence of patients developing a secondary ACS during a VOC. This study confirms that the PRESEV score could indeed represent a useful tool for physicians, most especially within emergency structures, by identifying patients with a low risk of further developing an ACS with a good NPV and thus, allowing a better management of SCD patients experiencing a VOC. The PRESEV score was successfully put to practice during the Covid-19 pandemic at the referral SCD center of Henri Mondor hospital and identified "low-risk" patients, who benefited from homecare services (DREPADOM). As such, the PRESEV score could represent a significant help when one considers the shortness of bed availabilities in certain circumstances (pandemics, hospital settings in resource-limited countries, etc...). Finally, the identification of "high-risk" patients could also become useful for improving the feasibility of clinical trials for the prevention of ACS.
Arlet:Novartis: Consultancy, Honoraria. Bartolucci:Novartis: Research Funding; Emmaus: Consultancy; Addmedica: Research Funding; Fabre Foundation: Research Funding; ADDMEDICA: Consultancy; HEMANEXT: Consultancy; AGIOS: Consultancy; Roche: Consultancy; Bluebird: Consultancy; Bluebird: Research Funding; Innovhem: Other; GBT: Consultancy; Novartis: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal